
CLICK HERE TO COMMENT
CLICK HERE TO SEE COMMENTS
Summary of Comments
•Maxillary swing would be a good approach:... Dr Mohnish Grover
•Radiotherapy or even better gamma knife excision can be excercised.:.. Dr Shashidhar
•Extended osteoplastic maxillotomy approach is very useful:... Dr Mercy George
•Drogenil tab to shrink it. Embolise for avascular.:... Dr Devan
•Approached via maxillary swing/preauricular subtemporal approach:...Dr Rohit Verma
•REPEAT SURGERY WITH RADICAL EXCISION AFTER INITIAL EMBOLIZATION... Dr Suneel
•Lateral skull base approach...need to drill vidian canal...proposed to be region for residual tumour...: ...Dr Rajeev
•Radiotherapy does help in such cases & after 1000 rads the mass almost disappear:...Dr Prakash Moonka
•Pre op angiography & embolization.trans septal approach to gain good access.remove posterior wall of maxilla , reach pterygopalatine fossa& medial part of infratemporal fossa enblock resection of the tumour....Dr Murthy
•Since lateral rhinotomy has been done twice ( medial maxillectomy would have been a part ) follow the same approach,, will prevent another scar: ...Dr Sarvejit
•Prepare a nasal corridor first with removal of the posterior half of nasal septum , followed by a wide antrostomy, then a caldwell luc opening , all these three wil give you a wide acess to the posterior wall of maxilla.... Dr B. Karthikeyan
. radio therapy..... Dr Mahendran
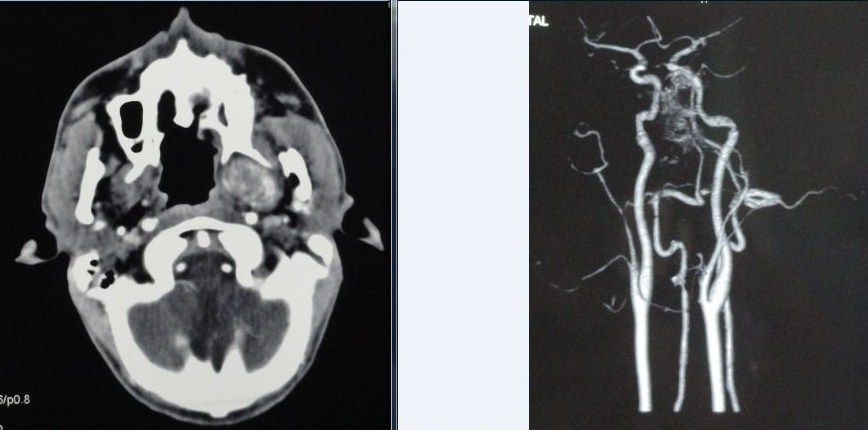
· In such type of disease to do before surgery site of origin extension"Fisch classification" of disease and possible blood vessel origin Ist to identify before surgery: Dr. Robiul Islam
· As recurrence involves the skull base,craniofacial approach with drilling the viridian canal to prevent recurrence should be the best…….Dr Ipsit Panda
· I think the best way is inject of sclrozan matter than transpalatal approch combind with endoscopic surgery……Dr Hassan Haidar
· The midfacial degloving approach, with or without a LeFort osteotomy, improves posterior access to the tumor.We can also finish the operation with endoscopy control…..Farid Boudjenah
· Pre-op embolisation,then proceed via an infratemporal approach……Dr jayita poduval
· By FESS…..wagie
· Combined intracranial and external approach - bicoronal frontal apporach, Considering for post operative Radiotherapy if any residual disease is suspected…….Dr S.Kamala Kannan
MS(ENT), DNB(ENT), MNAMS
Associate Professor(ENT)
Maulana Azad Medical College and associated Lok Nayak Hospital, New Delhi
If the dura is not involved and the mass is still extradural may be a maxillary swing would be useful. Ligation of the external carotid artery may be required.
ReplyDelete