Mouse over any of the cards to see the post title and comment count. As you scroll down, additional posts will continue to load.
Click on a card to see the post in full view. You can navigate through the posts using J (older post) and K (newer post) or the arrow keys. Hit escape or click Back to all posts to return to the Flipcard view.
In the upper left, click to sort by Date, Author and Category.
Click here to view
Thursday, 31 March 2011
Wednesday, 30 March 2011
RHINOCON 2011 ,April 28-29,Gangtok
24th Annual Conference of
All India Rhinology Society
RHINOCON 2011
Date :28th & 29th April, 2011
Venue Sikkim Manipal Institute of Medical
Sciences 5th Mile, Tadong,
Gangtok – 737102
Sikkim
www.smims.smu.edu.in
Email: rhinocongtk2011@gmail.com
VIEW DOWNLOAD BROCHURE
All India Rhinology Society
RHINOCON 2011
Date :28th & 29th April, 2011
Venue Sikkim Manipal Institute of Medical
Sciences 5th Mile, Tadong,
Gangtok – 737102
Sikkim
www.smims.smu.edu.in
Email: rhinocongtk2011@gmail.com
VIEW DOWNLOAD BROCHURE
APSCI 2011,October 25 to 28, 2011 at EXCO, Daegu, Korea
It is a great pleasure and honor for us to invite you to the forthcoming the 8th Asia Pacific Symposium on Cochlear Implant and Related Sciences (APSCI 2011) which will be held on October 25 to 28, 2011 at EXCO, Daegu, Korea. APSCI 2011 will be hosted by the department of Otorhinolaryngology, School of Medicine in Kyungpook National University which is the second oldest university in Korea.
APSCI 2011 is the international symposium for the exchange of information regarding research and development in Cochlear Implant and its related fields. We hope that you will take the unique opportunity to discuss your experience, interact with your colleagues and peers, and have a memorable and rewarding experience during your time in Daegu.
Website : http://www.apsci2011.kr/
Invited Faculty From India
Prof J M Hans( Delhi )
Prof Mohan Kameswaran ( Chennai)
APSCI 2011 is the international symposium for the exchange of information regarding research and development in Cochlear Implant and its related fields. We hope that you will take the unique opportunity to discuss your experience, interact with your colleagues and peers, and have a memorable and rewarding experience during your time in Daegu.
Website : http://www.apsci2011.kr/
Invited Faculty From India
Prof J M Hans( Delhi )
Prof Mohan Kameswaran ( Chennai)
Tuesday, 29 March 2011
Meeting & OTO EXPO will take place in San Francisco, California, USA, September 11-14, 2011.
Contact: Catherine R. Lincoln, CAE, MA
Senior Manager, International/Humanitarian
Email: international@entnet.org
Tel: 1-703-535-3738
Fax 1-703-299-1124
The American Academy of Otolaryngology—Head and Neck Surgery Foundation (AAO-HNSF) is pleased to announce that its next Annual Meeting & OTO EXPO will take place in San Francisco, California, USA. Please join us at the world’s largest gathering of the specialty, September 11-14, 2011.
Please post the following on your website or share it with your colleagues: The 2011 Call for Papers will be available at http://www.entnet.org/annual_meeting/callPapers2011.cfm where abstracts may be submitted:
• Miniseminars and Instruction Courses: submission opens November 8, 2010; deadline December 6, 2010; notification March 2011.
• Scientific Program: submission opens January 19, 2011; deadline February 14, 2011; notification May 2010.
Academy members enjoy special rates for meeting registration. To join, visit www.entnet.org/AboutUs/becomeMember.cfm or email memberservices@entnet.org for an application form.
Starting mid-May 2011, visit www.entnet.org for the latest Annual Meeting & OTO EXPO updates, or look in a spring issue of the Bulletin, which carries the preliminary program information. In May, registration and hotel reservations will be available online at www.entnet.org/annual__meeting.
Among special events for international registrants, are a reception and orientation for new members, Saturday, September 10, and an International Dessert Reception open to all international attendees and their spouses on Tuesday, September 13. International visitors are encouraged to wear their national dress or a flag lapel pin at the President’s Reception September 11 and at all evening receptions.
For attendees who need a U.S. visa, an invitation letter can be requested at no extra charge when registering online. The U.S. government recommends applying for a visa at least five months before arrival in the U.S.A. To learn more, visit http://www.unitedstatesvisas.gov/.
If you have questions, contact international@entnet.org. The Academy looks forward to welcoming you to the 2011 Annual Meeting & OTO EXPO, the world’s largest gathering of otolaryngologists—head and neck surgeons.
Senior Manager, International/Humanitarian
Email: international@entnet.org
Tel: 1-703-535-3738
Fax 1-703-299-1124
The American Academy of Otolaryngology—Head and Neck Surgery Foundation (AAO-HNSF) is pleased to announce that its next Annual Meeting & OTO EXPO will take place in San Francisco, California, USA. Please join us at the world’s largest gathering of the specialty, September 11-14, 2011.
Please post the following on your website or share it with your colleagues: The 2011 Call for Papers will be available at http://www.entnet.org/annual_meeting/callPapers2011.cfm where abstracts may be submitted:
• Miniseminars and Instruction Courses: submission opens November 8, 2010; deadline December 6, 2010; notification March 2011.
• Scientific Program: submission opens January 19, 2011; deadline February 14, 2011; notification May 2010.
Academy members enjoy special rates for meeting registration. To join, visit www.entnet.org/AboutUs/becomeMember.cfm or email memberservices@entnet.org for an application form.
Starting mid-May 2011, visit www.entnet.org for the latest Annual Meeting & OTO EXPO updates, or look in a spring issue of the Bulletin, which carries the preliminary program information. In May, registration and hotel reservations will be available online at www.entnet.org/annual__meeting.
Among special events for international registrants, are a reception and orientation for new members, Saturday, September 10, and an International Dessert Reception open to all international attendees and their spouses on Tuesday, September 13. International visitors are encouraged to wear their national dress or a flag lapel pin at the President’s Reception September 11 and at all evening receptions.
For attendees who need a U.S. visa, an invitation letter can be requested at no extra charge when registering online. The U.S. government recommends applying for a visa at least five months before arrival in the U.S.A. To learn more, visit http://www.unitedstatesvisas.gov/.
If you have questions, contact international@entnet.org. The Academy looks forward to welcoming you to the 2011 Annual Meeting & OTO EXPO, the world’s largest gathering of otolaryngologists—head and neck surgeons.
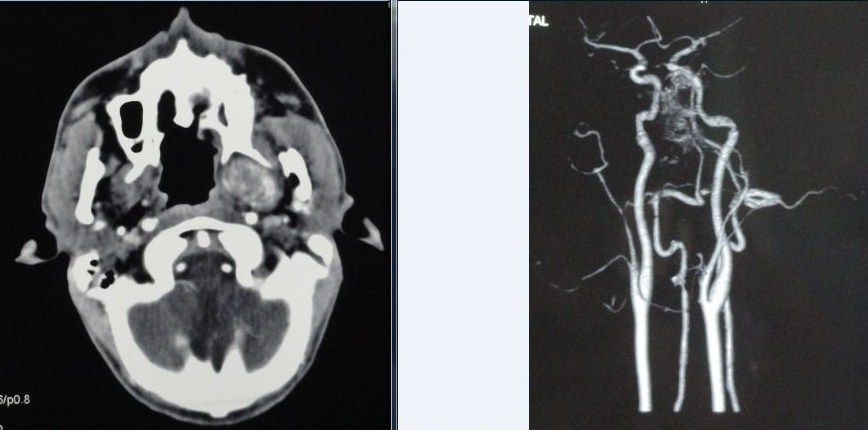
Imaging Tips:Cervical Adenopathy
- Regardless of lymph node size, most reliable imaging finding of metastatic disease is presence of central nodal necrosis on contrast-enhanced CT
- Nodes in jugulodigastric region (level II), or submandibular triangles (level I) with greater than 1.5 cm in maximum diameter, or node greater than 1 cm in maximum diameter elsewhere in neck, are considered likely to contain metastatic carcinoma
- In general, nodal enhancement seems to imply increased nodal vascularity, most common causes are acute infections
- Nodal calcification can be seen in metastatic nodes (papillary thyroid cancer, metastatic adenocarcinoma from lung, breast and gut) but may also be seen with tuberculosis, healed necrotic, abscessed nodes, amyloidosis
Monday, 28 March 2011

Sir Charles Bell
Sir Charles Bell (1774 - 1842), was a Scottish anatomist, neurologist, surgeon and natural theologian. He and his brother had remarkable artistic gifts, and together they taught anatomy and illustrated and published two volumes of A System of Dissection Explaining the Anatomy of the Human Body.

A number of discoveries received his name:
Bell's (external respiratory) nerve: The long thoracic nerve.
Bell's palsy: a unilateral idiopathic paralysis of facial muscles due to a lesion of the facial nerve.
Bell's phenomenon: An upward movement of the eye and the eyelid which occurs when a person affected with Bell's paralysis tries to close the eye.
Bell's spasm: Involuntary twitching of the facial muscles.
Bell-Magendie law or Bell's Law: States that the anterior branch of spinal nerve roots contain only motor fibers and the posterior roots contain only sensory fibers

A number of discoveries received his name:
Bell's (external respiratory) nerve: The long thoracic nerve.
Bell's palsy: a unilateral idiopathic paralysis of facial muscles due to a lesion of the facial nerve.
Bell's phenomenon: An upward movement of the eye and the eyelid which occurs when a person affected with Bell's paralysis tries to close the eye.
Bell's spasm: Involuntary twitching of the facial muscles.
Bell-Magendie law or Bell's Law: States that the anterior branch of spinal nerve roots contain only motor fibers and the posterior roots contain only sensory fibers
AOI Delhi State Conference 2011 Report

BM Abrol Trophy for AIIIMS(Best Clinical Meeting)
The 34th Annual Conference of Otolaryngologists Delhi State was held on 25th ,26th & 27th of March 2011.The Conference was attended by more than300 leading ENT doctors of Delhi & NCR.
Emenent doctors from Various parts of INDIA like Prof.Kirtane,Prof Pusalkar & Dr Meghnadh were invited to give guest orations on important topics.
The Conference started with Pre- Conference CME which was conducted by the Deptt.of ENT Sir Ganga Ram Hospital Laser assisted Surgical Techniques were shown & a case of Cochlear Implantation was demonstrated by Dr Anil Monga. Annual Conference was held on 26th & 27th at the PEIMER Auditorium of RML Hospital.
The Conference was inaugurated at a simple & elegant function by Padam Bhushan
Dr B K Rao chairman of Sir Ganga Ram Hospital.
During the course of the Conference, various academic activity like paper presentation for post gradutate students,Panel discussion by emenent ENT surgeons,Lecturesand
How i do it sessions were held.
Post Conference the General body discussed various issues facing the ENT surgeon.
Promenent issue was the formation of cartel by various Cochlear Implant Companies with few ENT Surgeons & refusal to supply the implant to highly trained & experieced ENT surgeons,thereby depriving their patients the benefit of Cochlear Implant.An unanimous Resolution was passed against the Restictive Trade Practives done by cochlear implant companies.
Dr Anoop Raj HOD MAMC stressed to first approach the companies & also to seek legal assistance if needed.
The Conference was sucessfully organized by:
Dr Anil K Monga-President
Dr Alok Agarwal-Organizing Secretary
Dr Manish Munjal-Treasurer
All 3 are consultants of the Deptt. of ENT Sir Ganga Ram Hospital.
Friday, 25 March 2011
ENT Quiz Round 9
CLICK HERE TO PARTICIPATE
Answer to Round 8
1]Surgery for glue ear is advised for a conductive loss equal to or more than D]30dB
3]The strain of HPV that causes malignant transformation in recurrent juvenile respiratory papillomatosis is B]11
2]The most reliable method of determining nasal airway obstruction is B]acoustic rhinomanometry
Total Responses 97
Correct Responders:
HAD3ENT MYSORE
GUDUPUDI VSKP
THADANIKHIL MANGALORE
PIYUSH DEHRADUN dr piyush tripathi
PARVAT SINGH SURATGARH Dr parvat singh shekhawt
DRUVENT CHENNAI Dr.U.Venkatesan
MOHAMMED SAYEER KANNUR Dr.Mohammed Sayeer
SHAKEELAMU LUCKNOW DR MOHAMMAD SHAKEEL
KHALIDMAHIDA KARACHI PAKISTAN DR KHALIDMAHIDA
DRJEWELMMCH DHAKA
Answer to Round 8
1]Surgery for glue ear is advised for a conductive loss equal to or more than D]30dB
3]The strain of HPV that causes malignant transformation in recurrent juvenile respiratory papillomatosis is B]11
2]The most reliable method of determining nasal airway obstruction is B]acoustic rhinomanometry
Total Responses 97
Correct Responders:
HAD3ENT MYSORE
GUDUPUDI VSKP
THADANIKHIL MANGALORE
PIYUSH DEHRADUN dr piyush tripathi
PARVAT SINGH SURATGARH Dr parvat singh shekhawt
DRUVENT CHENNAI Dr.U.Venkatesan
MOHAMMED SAYEER KANNUR Dr.Mohammed Sayeer
SHAKEELAMU LUCKNOW DR MOHAMMAD SHAKEEL
KHALIDMAHIDA KARACHI PAKISTAN DR KHALIDMAHIDA
DRJEWELMMCH DHAKA
"CONVENTIONAL AND ENDOSCOPIC PHONOSURGERY WORKSHOP" on April 2-3,2011 Hyderabad
We are glad to update you the preperations for the upcoming "CONVENTIONAL AND ENDOSCOPIC PHONOSURGERY WORKSHOP" on April 2-3,2011 at Hotel Taj Deccan,Hyderabad.
We are happy to inform you that we could collect a number of cases comprising a whole variety of voice pathologies totaling 20 in number.
This is a list of the cases which we are planning to operate during the workshop
1. Unilateral vocal cord palsy
2. Bilateral vocal cord palsy
3. Vocal polyps
4. vocal nodules
5. Sulcus vocalis
6. Reinkes oedema
7. Puberophonia
8. Laryngeal paillomatosis
9. Spasmodic dysphonia
We are planning to demonstrate comprehensive methods in Phonosurgery to take care of various voice problems which include
1. Newer techniques in medialization thyroplasty
2. Fibreoptic endolaryngeal phonosurgery
3. Endoscopic phonosurgery
4. Type III thyroplasty
kindly keep your dates free for the workshop.
Thanking you.
Dr M.Mohan Reddy,
Organizing secretary.
novaenthospital@gmail.com
We are happy to inform you that we could collect a number of cases comprising a whole variety of voice pathologies totaling 20 in number.
This is a list of the cases which we are planning to operate during the workshop
1. Unilateral vocal cord palsy
2. Bilateral vocal cord palsy
3. Vocal polyps
4. vocal nodules
5. Sulcus vocalis
6. Reinkes oedema
7. Puberophonia
8. Laryngeal paillomatosis
9. Spasmodic dysphonia
We are planning to demonstrate comprehensive methods in Phonosurgery to take care of various voice problems which include
1. Newer techniques in medialization thyroplasty
2. Fibreoptic endolaryngeal phonosurgery
3. Endoscopic phonosurgery
4. Type III thyroplasty
kindly keep your dates free for the workshop.
Thanking you.
Dr M.Mohan Reddy,
Organizing secretary.
novaenthospital@gmail.com
Tuesday, 22 March 2011
http://www.sinusvideos.com/
SinusVideos.com intends to provide high quality videos of sinus surgeries for the educational benefit of healthcare providers and their patients. New videos are continually being added and many have links to supplemental text and diagrams describing additional details of the surgery. We hope you enjoy the site and will share your comments with us at editors@sinusvideos.com.
Ralph Metson M.D.
Clinical Professor and Rhinology Fellowship Director
Harvard Medical School
Zachary Soler M.D.
Rhinology Fellow (former)
Harvard Medical School
Jamie Litvack M.D., M.S.
Rhinology Fellow (current)
Harvard Medical School
Monday, 21 March 2011
Recovery Position
All forms of the recovery position share basic principles. The mouth is downward so that fluid can drain from the patient's airway; the chin is well up to keep the epiglottis opened. Arms and legs are locked as to stabilize the position of the patient
Saturday, 19 March 2011
“Don’t be a turbinator!”
“Empty nose syndrome (ENS), also known as ‘the wide nasal cavity syndrome,’ is a term coined by Dr. Eugene Kern of the Mayo Clinic (1994) to describe a rare and debilitating iatrogenic syndrome of chronic nasal physiological impairment following overzealous turbinate resections in the nose (turbinectomies).”
There is a growing disagreement that Empty Nose Syndrome is a rare condition. With approximately half a million turbinate reductions being performed yearly just in the United States, and an increasing outcry from injured patients, it is now suspected that injuries may number in the millions worldwide.
34th Annual Conference 2011 of the Association of Otolaryngologists of India DELHI BRANCH 26th - 27th March, 2011
VENUE
PGIMER Auditorium
Dr Ram Manohar Lohia Hospital,
Visit us at: www.aoidelhi.net
Dr.Alok Agarwal
5/11,
New Delhi-110008
MOB: +91-9811211667
Friday, 18 March 2011
ENT Quiz Round 8
Answer to Round 7
1]The principal reason for retraction of the malleus handle in cases of CSOM with perforation is- D]unopposed action of the tensor tympani
2]All are true for antrochoanal polyp except C]the maxillary ostium is constricted
3]Quincke’s oedema is A]angioneurotic oedema of the uvula
Summary Implant materials in augmentation rhinoplasty
Implant materials in augmentation rhinoplasty
A. Autograft : Cartilage, Bone, Fascia and Dermis
B. Homograft: Cartilage, Bone : Preserved, irradiated or lyophilized.
C. Xenograft : Porcine/ Bovine collagen : They are often reabsorbed and replaced with variable
deposition of host’s fibrous tissues.
SYNTHETIC: (Alloplasts)
Silicone (Silastic)
Polyethylene (Medpore)
Polyamide mesh
Polytetrafluroethylene : eg: Gore-tex, Proplast
Fillers : Used For Non-Surgical Rhinoplasty
Temporary fillers:
1.Calcium hydroxyapatite-based fillers e.g. Radiesse (lasts upto 1 year)
i.Hyaluronic acid-based fillers e.g. Juvederm (Lasts upto 6-8 months)
ii.Liquid silicone (Not FDA-approved as cosmetic facial filler)
iii.Permanent fillers:
2.
• Polymethylmethacrylate (PMMA ) beads . eg : Artefill
Artefill is the only currently FDA-approved permanent filler
Dr Ipsit Panda(Delhi)
Thursday, 17 March 2011
Impact on hearing of routine ear suctioning at the tympanic membrane
Am J Otolaryngol. 2011 Mar-Apr;32(2):100-4. Epub 2010 Apr 13.
Impact on hearing of routine ear suctioning at the tympanic membrane.
Nelson JJ, Giraud A, Walsh R, Mortelliti AJ.
Abstract
OBJECTIVE: Patient and equipment safety has become increasingly scrutinized in today's medical care. Routine otolaryngologic evaluation often involves suctioning with Frazier-type suction devices in the ear canal for improved visualization, but data are limited on the potential acoustic trauma from ear canal suction devices. This study intends to document the objective and subjective effects of ear canal suctioning to identify any risk for hearing threshold shifts or other potential negative effects.
PATIENTS AND METHODS: Prospective study on 21 healthy volunteers enlisted for evaluation. Presuctioning tympanogram, audiogram, and otoacoustic emissions data were obtained. Spectrum analyses were recorded during ear canal suctioning with a probe microphone placed lateral to the tympanic membrane. Subjective data were recorded, and a follow-up audiogram and otoacoustic emissions were obtained to identify any temporary threshold shifts.
RESULTS: Spectrum analyses revealed a high degree of variability between subjects. A peak intensity of 111 dB sound pressure level was recorded. All patients tolerated suctioning, and none reported hearing loss. No threshold shifts were observed. Subjective data failed to correlate with the objective recorded intensities.
CONCLUSIONS: Clinicians and patients need to be acutely aware of potential risks and benefits from any medical intervention. Routine ear canal suctioning can be extremely loud and uncomfortable for patients. This study failed to document objective proof of hearing detriment from ear canal suctioning, although the possibility exists during office and surgical intervention. Further study and potential alternative suctioning methods deserve attention.
Monday, 14 March 2011

Readers Forum 2: Recurrence of Angiofibroma

CLICK HERE TO COMMENT
CLICK HERE TO SEE COMMENTS
Summary of Comments
•Maxillary swing would be a good approach:... Dr Mohnish Grover
•Radiotherapy or even better gamma knife excision can be excercised.:.. Dr Shashidhar
•Extended osteoplastic maxillotomy approach is very useful:... Dr Mercy George
•Drogenil tab to shrink it. Embolise for avascular.:... Dr Devan
•Approached via maxillary swing/preauricular subtemporal approach:...Dr Rohit Verma
•REPEAT SURGERY WITH RADICAL EXCISION AFTER INITIAL EMBOLIZATION... Dr Suneel
•Lateral skull base approach...need to drill vidian canal...proposed to be region for residual tumour...: ...Dr Rajeev
•Radiotherapy does help in such cases & after 1000 rads the mass almost disappear:...Dr Prakash Moonka
•Pre op angiography & embolization.trans septal approach to gain good access.remove posterior wall of maxilla , reach pterygopalatine fossa& medial part of infratemporal fossa enblock resection of the tumour....Dr Murthy
•Since lateral rhinotomy has been done twice ( medial maxillectomy would have been a part ) follow the same approach,, will prevent another scar: ...Dr Sarvejit
•Prepare a nasal corridor first with removal of the posterior half of nasal septum , followed by a wide antrostomy, then a caldwell luc opening , all these three wil give you a wide acess to the posterior wall of maxilla.... Dr B. Karthikeyan
. radio therapy..... Dr Mahendran
.Difficult case indeed. Will need a combined infra temporal fossa and endoscopic approach to the pterygopalatine fossa...Dr V Ravi Kumar
· In such type of disease to do before surgery site of origin extension"Fisch classification" of disease and possible blood vessel origin Ist to identify before surgery: Dr. Robiul Islam
· As recurrence involves the skull base,craniofacial approach with drilling the viridian canal to prevent recurrence should be the best…….Dr Ipsit Panda
· I think the best way is inject of sclrozan matter than transpalatal approch combind with endoscopic surgery……Dr Hassan Haidar
· The midfacial degloving approach, with or without a LeFort osteotomy, improves posterior access to the tumor.We can also finish the operation with endoscopy control…..Farid Boudjenah
· Pre-op embolisation,then proceed via an infratemporal approach……Dr jayita poduval
· By FESS…..wagie
· Combined intracranial and external approach - bicoronal frontal apporach, Considering for post operative Radiotherapy if any residual disease is suspected…….Dr S.Kamala Kannan
Opinion may differ from surgeon to surgeon. some may prefer to operate via endoscopic or open approach depending upon the expertise, but preoperative embolisation is imporant and drilling of the vidian canal is a must to prevent the recurrence. The intracranial part is almost always extradural and may come out totally but if there is any residual intracranial part if any can be dealt by Gamma knife post operatively.
Dr Ravi Meher
MS(ENT), DNB(ENT), MNAMS
Associate Professor(ENT)
Maulana Azad Medical College and associated Lok Nayak Hospital, New Delhi
MS(ENT), DNB(ENT), MNAMS
Associate Professor(ENT)
Maulana Azad Medical College and associated Lok Nayak Hospital, New Delhi
13th International Otology Course,Causse Clinique,June 30-July 2,2011
This 3-day course is dedicated to live surgery, conference and panel discussion on otosclerosis, ossicular reconstruction, cholesteatoma surgery, middle ear implant, cochlear implant and neurotology.
The 13 live surgery sessions will demonstrate the techniques used at the Causse Ear Clinic. Recent advances such as malleus replacement prosthesis and new original techniques will be demonstrated.
You can register on-line or download the registration form at http://clinique-causse.com/course2011/registration/. There is a limited number of available place.
A pre-course invitation is extended to colleagues who wish to visit the Causse Ear Clinic for a period of their choice prior to the 13th Otology Course. They will join clinic surgeons observing live surgery in an intimate and academically stimulating atmosphere. The group will be limited to a maximum of 15 persons on a "first come first served basis". Please contact Stéphanie Ros by e-mail, by phone (+33 4 67 35 63 95) or by fax (+33 4 67 35 62 00)
The 13th Otology Course will be broadcasted in live streaming via the LION network. To follow the Course go to http://clinique-causse.com/course2011/live_surgery.html and click on "Live on the Web".
For more information please go to: http://www.clinique-causse.com/course2011
The 13 live surgery sessions will demonstrate the techniques used at the Causse Ear Clinic. Recent advances such as malleus replacement prosthesis and new original techniques will be demonstrated.
You can register on-line or download the registration form at http://clinique-causse.com/course2011/registration/. There is a limited number of available place.
A pre-course invitation is extended to colleagues who wish to visit the Causse Ear Clinic for a period of their choice prior to the 13th Otology Course. They will join clinic surgeons observing live surgery in an intimate and academically stimulating atmosphere. The group will be limited to a maximum of 15 persons on a "first come first served basis". Please contact Stéphanie Ros by e-mail, by phone (+33 4 67 35 63 95) or by fax (+33 4 67 35 62 00)
The 13th Otology Course will be broadcasted in live streaming via the LION network. To follow the Course go to http://clinique-causse.com/course2011/live_surgery.html and click on "Live on the Web".
For more information please go to: http://www.clinique-causse.com/course2011

Hands on Basic Temporal Bone Dissection Course,29 th April - 1 May,2011,Hyderabad, India

Contact : drchaitanya@raosentcare.com
Saturday, 12 March 2011

Friday, 11 March 2011
ENT Quiz Round 7
ROUND 7
Round 6 Answers
1]Acquired cholesteatoma is believed to first develop in B]Prussak’s space
2]Hebra nose is seen in D]rhinoscleroma
3]To define OSAsyndrome,apnoea-hypapnoea index should be = or > A]5
Correct Responders
Dr Anshul/Delhi
Dr Ajay/ Mangalore
Dr Mohnish/Jaipur
Dr Ipsit/Delhi
Dr Rajeev/Delhi
Dr Parvat Sungh/Suratgarh
Dr Anuj/Chennai
Spot The Dx -Thyroglossal Duct Cyst with Thyroid Ectopia

Thyroid Scan shows no radiotracer uptake in Thyroid Bed.
Uptake is in mass above Hyoid Shown above.
TSH raised .
121 Responders
CLICK HERE TO SEE RESPONSES
CLICK HERE TO SEE RESPONSES
Dr Zakir from Peshawer was first correct responder.
Thursday, 10 March 2011
Cranial Nerves-Trivia
Longest intracranial course -- trochlear n.
Longest extracranial course --vagus n.
Largest and thickest -- trigeminal n.
CN with dorsal exit -- trochlear n.
CN which is the smallest -- olfactory n.
Abducent nerve has the longest intra-cranial SUB-ARACHNOID course!!
Longest extracranial course --vagus n.
Largest and thickest -- trigeminal n.
CN with dorsal exit -- trochlear n.
CN which is the smallest -- olfactory n.
Abducent nerve has the longest intra-cranial SUB-ARACHNOID course!!
Tuesday, 8 March 2011
ENT Quiz Round 1 & 2
We are thankful to Readers for massive & Worldwide response to Quiz section.
The new Quiz is floated at week ends only.
The Round 1 and Round 2 were carried out earlier in Poll format without recording the individual readers response .
We are floating these Rounds again in recent format.
CLICK LINKS BELOW TO PARTICIPATE
ENT QUIZ ROUND 1
ENT QUIZ ROUND 2
Quiz Master
Dr Jayita Poduval
Associate Professor
Department Of ENT
AIMST University
Kedah Darul Alam
Malaysia
The new Quiz is floated at week ends only.
The Round 1 and Round 2 were carried out earlier in Poll format without recording the individual readers response .
We are floating these Rounds again in recent format.
CLICK LINKS BELOW TO PARTICIPATE
ENT QUIZ ROUND 1
ENT QUIZ ROUND 2
Quiz Master
Dr Jayita Poduval
Associate Professor
Department Of ENT
AIMST University
Kedah Darul Alam
Malaysia
NAPST 2011 SLEEP CONFERENCE,July 2-3, 2011,Kuala Lumpur
NAPST 2011 SLEEP CONFERENCE
Network of Asia-Pacific Sleep Technologists
July 2-3, 2011
This is the third bi-annual conference offering lectures and courses on sleep medicine and technology in
the Asia-Pacific region. We anticipate attendees from across the Asia Pacific region and Middle East.
The NAPST Organizing Committee welcomes your participation in this event to foster new ties and
relationships, share developments in the respective countries, and highlight the growing importance of
the Sleep Disorders profession throughout Asia. This conference will be approved for CECs from the
American Association of Sleep Technologists (AAST).
Dr. Anitha Vivekanandan.
ORL Specialist, UiTM,Mala.
Contact No:+6012-480057
For more details and registration information,
email: dan@sleep-asia.com or visit
www.napst.wordpress.com
Network of Asia-Pacific Sleep Technologists
July 2-3, 2011
This is the third bi-annual conference offering lectures and courses on sleep medicine and technology in
the Asia-Pacific region. We anticipate attendees from across the Asia Pacific region and Middle East.
The NAPST Organizing Committee welcomes your participation in this event to foster new ties and
relationships, share developments in the respective countries, and highlight the growing importance of
the Sleep Disorders profession throughout Asia. This conference will be approved for CECs from the
American Association of Sleep Technologists (AAST).
Dr. Anitha Vivekanandan.
ORL Specialist, UiTM,Mala.
Contact No:+6012-480057
For more details and registration information,
email: dan@sleep-asia.com or visit
www.napst.wordpress.com
Sunday, 6 March 2011
ENDOSCOPIC COLOR ATLAS OF EAR DISEASES. M M Khan, S R Parab

ENDOSCOPIC COLOR ATLAS OF EAR DISEASES. M M Khan, S R Parab. Jaypee Brothers Medical Publishers, 2011 ISBN 13 978 93 5025 166 9 pp 190. Price £65
READ REVIEW ....
Friday, 4 March 2011
ENT Quiz Round 6
CLICK HERE TO PARTICIPATE
Answers to Quiz Round 5
1]The nerve with the longest intracranial course is the A]trochlear
2]The stage in which the tensor veli palatini muscle is involved in opening of the Eustachian tube is D]third and fourth
3]The most common site for a torus mandibularis is B]opposite the canine and premolars
Winner : Dr J P ,Ahmedabad
Answers to Quiz Round 5
1]The nerve with the longest intracranial course is the A]trochlear
2]The stage in which the tensor veli palatini muscle is involved in opening of the Eustachian tube is D]third and fourth
3]The most common site for a torus mandibularis is B]opposite the canine and premolars
Winner : Dr J P ,Ahmedabad
Tuesday, 1 March 2011
PHON0CON 2011 Pics

A great event in all aspects.
This is not the first time that Col WVBS Ramalingam and Lt Col Rakesh Datta have worked together. From medialisation thyroplasties to attending conferences, their team forms a formidable duo. Now they got together to bring to you PHONOCON 2011, a prestigious academic gathering of professionals dealing with voice disorders.
A job well done.
Medial fracturing of the inferior turbinate: effect on the ostiomeatal unit and the uncinate process.
Eur Arch Otorhinolaryngol. 2009 Jun;266(6):857-61. Epub 2008 Nov 8.
Medial fracturing of the inferior turbinate: effect on the ostiomeatal unit and the uncinate process.
Lee KC, Lee SS, Lee JK, Lee SH.
Department of Otolaryngology, Kangbuk Samsung Medical Center, Sungkyunkwan University School of Medicine, 108, Pyoung-Dong, Jongro-Ku, Seoul, 110-746, South Korea.
Abstract
It is apparently a common practice to fracture the inferior turbinate medially and superiorly to facilitate the fenestration of the inferior meatus, and to fracture medially and lateralize the inferior turbinate during turbinoplasty. However, it is also known that medial fracturing of the inferior turbinate may induce lateral displacement of the uncinate process. We investigated medial fracturing of the inferior turbinate to see whether it had any effect on changing the position of the uncinate process. A retrospective study was done on 23 patients who underwent medial fracturing of the inferior turbinate during submucosal turbinoplasty or turbinectomy from January 2004 through September 2006. By analyzing ostiomeatal-unit computed tomography, we measured the angle of the uncinate process, the minimal width of the ethmoid infundibulum, and the size of the maxillary sinus ostium. The angle of the uncinate process was 14.19-32.45 degrees , the minimal width of the ethmoid infundibulum was 0.61-2.45 mm, and the size of the maxillary sinus ostium was 2.14-6.77 mm. After the surgery, the angle of the uncinate process was 15.56-32.51 degrees , the minimal width of the ethmoid infundibulum was 0.53-2.52 mm, and the size of the maxillary sinus ostium was 2.18-7.01 mm. Pathologic change in the ostiomeatal-unit was not observed for an average period of 14.9 months (range 10.3-21.8 months) follow-up period. Our report suggests that the medial fracturing of the inferior turbinate does not alter the position of the uncinate process and the size of the maxillary sinus ostium. Clinically, it does not seem to affect normal physiology of the sinus function nor does it cause sinusitis.
Medial fracturing of the inferior turbinate: effect on the ostiomeatal unit and the uncinate process.
Lee KC, Lee SS, Lee JK, Lee SH.
Department of Otolaryngology, Kangbuk Samsung Medical Center, Sungkyunkwan University School of Medicine, 108, Pyoung-Dong, Jongro-Ku, Seoul, 110-746, South Korea.
Abstract
It is apparently a common practice to fracture the inferior turbinate medially and superiorly to facilitate the fenestration of the inferior meatus, and to fracture medially and lateralize the inferior turbinate during turbinoplasty. However, it is also known that medial fracturing of the inferior turbinate may induce lateral displacement of the uncinate process. We investigated medial fracturing of the inferior turbinate to see whether it had any effect on changing the position of the uncinate process. A retrospective study was done on 23 patients who underwent medial fracturing of the inferior turbinate during submucosal turbinoplasty or turbinectomy from January 2004 through September 2006. By analyzing ostiomeatal-unit computed tomography, we measured the angle of the uncinate process, the minimal width of the ethmoid infundibulum, and the size of the maxillary sinus ostium. The angle of the uncinate process was 14.19-32.45 degrees , the minimal width of the ethmoid infundibulum was 0.61-2.45 mm, and the size of the maxillary sinus ostium was 2.14-6.77 mm. After the surgery, the angle of the uncinate process was 15.56-32.51 degrees , the minimal width of the ethmoid infundibulum was 0.53-2.52 mm, and the size of the maxillary sinus ostium was 2.18-7.01 mm. Pathologic change in the ostiomeatal-unit was not observed for an average period of 14.9 months (range 10.3-21.8 months) follow-up period. Our report suggests that the medial fracturing of the inferior turbinate does not alter the position of the uncinate process and the size of the maxillary sinus ostium. Clinically, it does not seem to affect normal physiology of the sinus function nor does it cause sinusitis.
The 59th hands on cadaver FESS workshop conducted by Dr.Raos
The 59th hands on cadaver FESS workshop conducted by Dr.Raos ENT super specialty hospital headed by Dr.G.V.S Rau under the auspices of Hyderabad ENT Research foundation was a grand success. it had more than 20 delegates in attending from all over the world and India.. there were 7 course-co ordinators present all along during hands on cadaver FESS of each participant guiding them through out the procedure.many of the delegates said that it was an educational feast on FESS and day after day, they learnt overwhelming amounts of knowledge regarding FESS. a Delegate from Nagpur says "it is one of the best workshops i have attended in my life", one from Syria says "this workshop has been of great help to me in understanding FESS, i will recommend this workshop to all my colleagues in Egypt"
It started with wide variety of lectures on anatomy surgical, endoscopic and radiological followed by demonstration of the intricate details of FESS on a fresh cadaver starting from the very basic details about instrumentation to the complications and how to tackle and prevent them from occurrence.
it was followed by live surgeries starting from the most basic polypectomies to the fungal sinusitis invading the orbit and intracranial cavity. the demonstration was done with basic instrumentation on one side and powered instruments on other side to show the difference. the three guest faculties showed different techniques of doing FESS. third day had lectures on advanced FESS.
We take this oppurunity specially thank Dr.Karla of www.entindia.net, Dr. Soni, Dr.krishna Kishore, Dr.Venkat Ram Reddy, Dr.Sai Raj, Dr. Arun Kumar, Dr.Krishna Reddy, Dr.Anoop for their active participation in making this workshop gain such heights.
The videos of the demonstration including some of the demonstration will be uploaded on Youtube channel www.youtube.com/raosentcare, www.raosentcare.com. we look forward to the next workshop on 60th Hands on Temporal Bone Dissection in the ending of April.
For more details please write to us at drchaitanya@raosentcare.com.
It started with wide variety of lectures on anatomy surgical, endoscopic and radiological followed by demonstration of the intricate details of FESS on a fresh cadaver starting from the very basic details about instrumentation to the complications and how to tackle and prevent them from occurrence.
it was followed by live surgeries starting from the most basic polypectomies to the fungal sinusitis invading the orbit and intracranial cavity. the demonstration was done with basic instrumentation on one side and powered instruments on other side to show the difference. the three guest faculties showed different techniques of doing FESS. third day had lectures on advanced FESS.
We take this oppurunity specially thank Dr.Karla of www.entindia.net, Dr. Soni, Dr.krishna Kishore, Dr.Venkat Ram Reddy, Dr.Sai Raj, Dr. Arun Kumar, Dr.Krishna Reddy, Dr.Anoop for their active participation in making this workshop gain such heights.
The videos of the demonstration including some of the demonstration will be uploaded on Youtube channel www.youtube.com/raosentcare, www.raosentcare.com. we look forward to the next workshop on 60th Hands on Temporal Bone Dissection in the ending of April.
For more details please write to us at drchaitanya@raosentcare.com.
Subscribe to:
Comments (Atom)